
TENDINOPATÍA ROTULIANA
Patellar tendinopathy is any clinical picture derived from an overload mechanism that affects the patellar tendon and the structures that surround it. The most characteristic symptoms of patellar tendinopathy are pain, inflammation (diffuse or localized), and functional impotence. Tendinopathies can occur due to tendinosis, tendonitis, paratendinitis, enthesopathies. This type of injury is characterized by the appearance of delayed pain produced by a series of tissue changes that make the injury chronic. Therefore, the pain produced by the injury prevents proper functionality. In the supposed practical case that we will discuss later, it will consist of reducing pain or eliminating it completely while squatting.
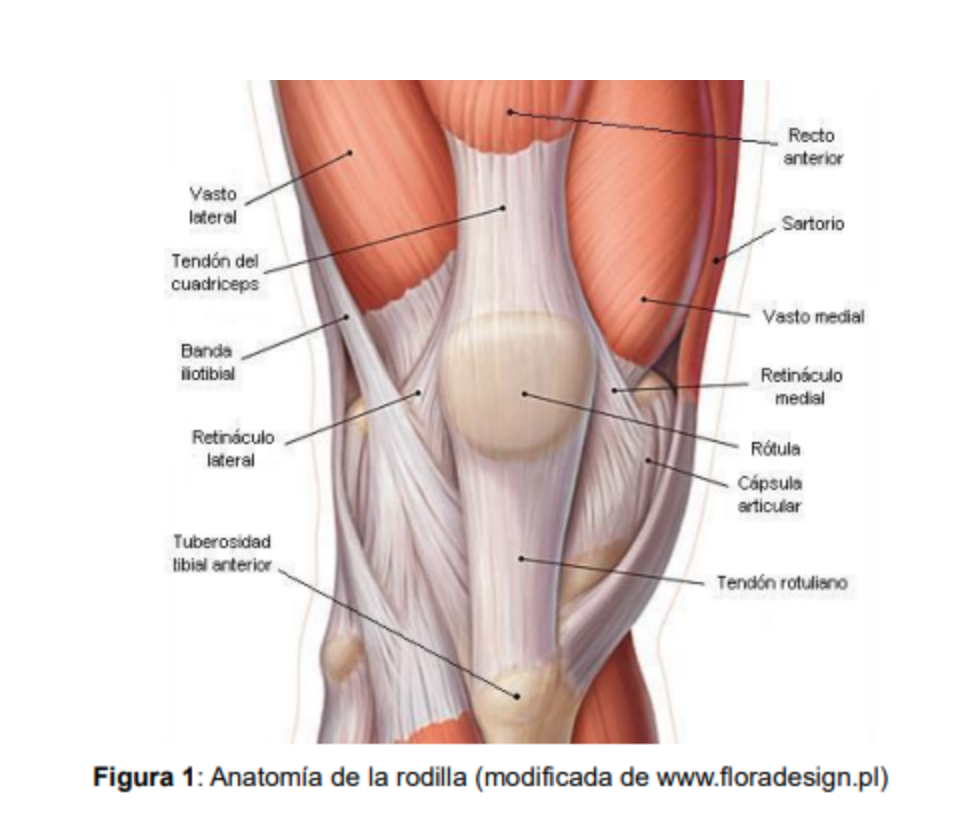
ROTULIAN TENDON
Tendons are structures composed of 30% collagen, 2% elastin and 68% water that are located between the muscle and the bone with the function of transmitting the force produced in the muscle belly until its insertion in the bone to produce the desired movement.
The tendon is divided into three specific zones:
- Musculotendinous union: It is an area where the tendon joins the muscle, with a certain capacity for stretching and is rarely affected by tendinopathies.
- Tendon-bone union: Area where four transition zones meet where the tendon inserts into the bone.
- Middle zone: Middle part of the tendon, it is practically the entire structure of the tendon.
Vascularization is scarce and this vascularity is more deficient in men than in women and decreases with age and mechanical overload. However, the blood supply of the tendon increases during exercise due to the healing processes. Being subjected to continuous stress makes you susceptible to injury very frequently.
TENDINOPHATY FACTORS
- Intrinsic factors: One of the responsible factors may be overuse exhaustion, which leads to muscle stiffness with a decrease in the extensibility of the muscle-tendon complex and a lesser capacity for rapid contraction that increases the traction on the patellar tendon.
- Extrinsic factors: Most authors agree that the misapplication of training loads may be the main culprit in terms of the appearance of patellar tendinopathy as the main external factor.
INTERVENTION
In this intervention we will perform an inhibition in the quadriceps to release tension in the patellar tendon by applying an electrostimulation protocol that in turn will produce a deformation in the red blood cells and an increase in nitric oxide synthase [1] to improve the blood vascularization of the tendon ; improve the physical conditions of the tendon [2,3] if there has been any tendinopathy and inhibit the stimulation of pain. In this way the subject will be able to train without discomfort and without suffering a greater risk of injury.
PHASE 1
We will place the whole-body electrostimulation on the subject in standing position. We will connect electrostimulation with a protocol of 80 Hz frequency with 350 microseconds of pulse width with 4 seconds of electrical impulse time and 2 seconds of rest. The intensity of WB-EMS will only increase in the quadriceps up to a motor threshold. The subject will have to contract the quadriceps during the electrical impulse and relax it at rest. The series will last 60 seconds.
PHASE 2
Once phase 1 is finished, we will carry out the same process as in phase 1 with a WB-EMS protocol of 40 Hz frequency with 300 microseconds of pulse width, the intensity remains at a motor threshold and the duty cycle will be 60 seconds of electrical impulse. During the electrical impulse the subject will perform a voluntary contraction of the quadriceps.
PHASE 3
In this phase the subject will perform squats with a WB-EMS protocol of 40 Hz frequency with 300 microseconds of pulse width, the intensity remains at a motor threshold and the duty cycle of the electrical impulse will be 25 seconds of work and 5 seconds seconds of rest. While the subject executes the squat (90º), we will increase the intensity of the hamstring causing a reciprocal inhibition of the quadriceps, relaxing said muscle exogenously and in turn causing a decrease in tension of the patellar tendon. We will carry out four work cycles.
At the end of the entire process of the three parts as the final phase, we will apply phase 1 and phase 2. To achieve an inhibition of the quadriceps, causing a decrease in tendon tension, thus reducing the pain stimulus and finally causing a greater vascularization of the patellar tendon by increasing nitric oxide synthase and better tendon regeneration.
EFFECT OF WB-EMS ON CHEMICAL PROCESSES RELATED TO PAIN.
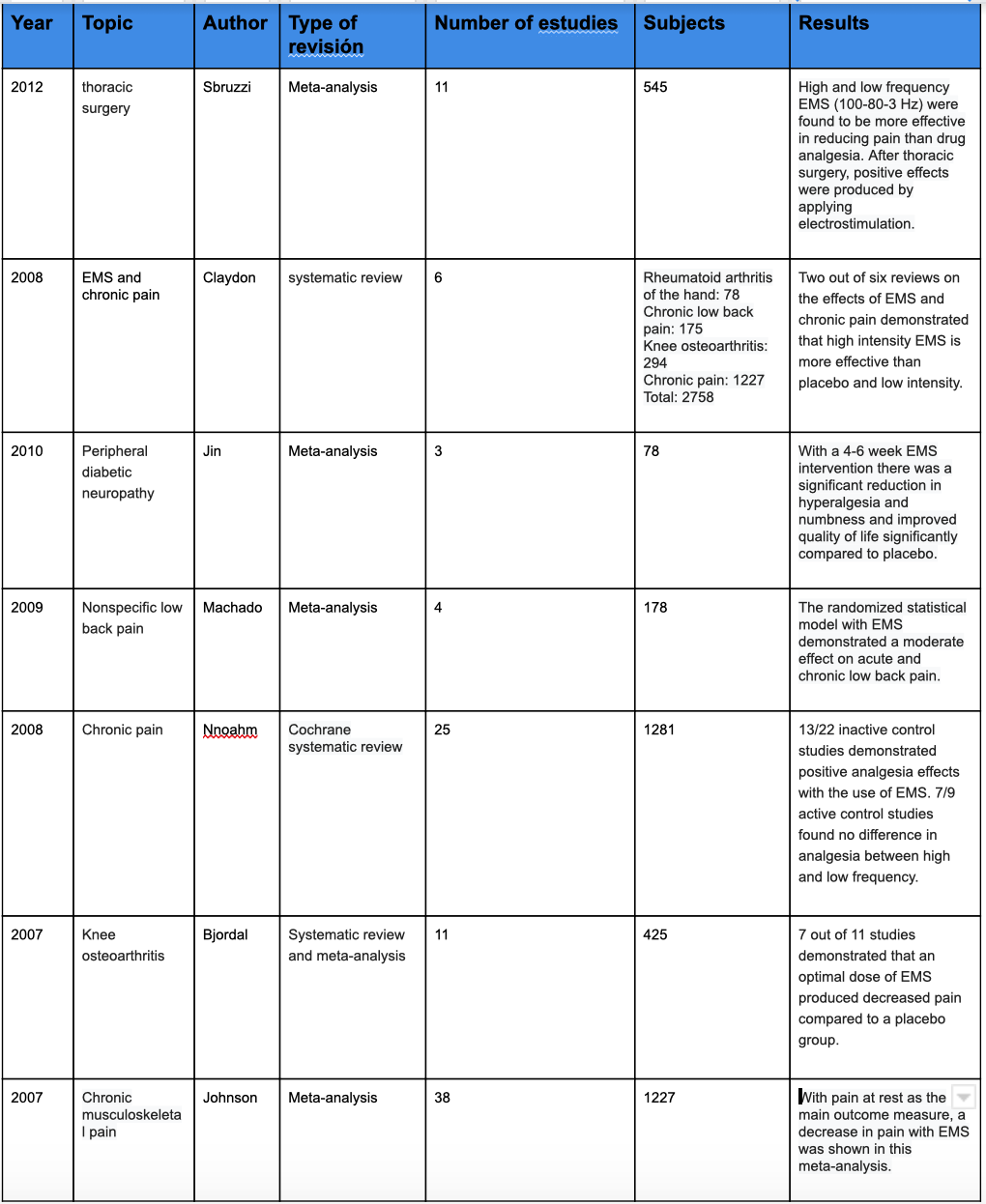
If we delve into the reviews mentioned in the table, high-frequency EMS (100 Hz) increases the concentration of β-endorphins and this can generate an analgesic effect in terms of a pain stimulus. On the other hand, the use of low frequency can produce physiological alterations such as an increase in serotonin among others, and this can give us a positive effect to reduce pain.
NUTRITIONAL STRATEGY PRE AND POST-INTERVENTION
Before and after performing the intervention, we could advise the specific consumption of certain nutritional substances that can help us improve performance at the joint level.
1. Pre-intervention nutritional supplementation:
- ß-Alanine: It is a non-essential amino acid synthesized by the liver that can be ingested through the diet (sources of animal origin) or through nutritional supplements. This non-essential amino acid has gained great interest due to its direct relationship with the synthesis of carnosine. The most important functions related to the ability to act as a powerful buffer at the muscle level, as well as the improvement in the sensitivity of calcium at the level of the muscle fiber. This last benefit can act as a muscle protective mechanism.
- Arginine: It is a semi-essential amino acid that is responsible for the production of nitric oxide, nitric oxide is produced from arginine by the enzyme nitric oxide synthase in many tissues and in the vascular endothelium it behaves as a vasodilator. On the other hand, the existence of an endogenous inhibitor of nitric oxide synthase called dimethylarginineasymmetric has been demonstrated. This compound is responsible for reducing the formation of nitric oxide produced by arginine. Therefore, arginine supplementation is important to counteract this effect.
- Vitamin C and hydrolyzed collagen: Supplementation with gelatin enriched with vitamin C (15gr) and hydrolyzed collagen can improve collagen synthesis when taken 1 hour before exercise. Therefore, it could be very helpful for tendon healing as 30% of the tendon is made up of collagen.
2. Post-intervention nutritional supplementation:
- Curcuma: Curcumin is the main active component of turmeric, a yellow compound originally isolated from the Curcuma longa plant. There is some evidence showing that turmeric has anti-inflammatory activities. Therefore, after the intervention, the consumption of turmeric would be a great help.
BIBLIOGRAPHY:
- Andre Filipovic, Heinz Kleino¨Der, Denise Plu¨Ck, Wildor Hollmann, Wilhelm Bloch, and Marijke Grau. (2015). Influence of Whole-Body Electrostimulation on Human Red Blood Cell Deformability. Journal of Strength and Conditioning Research, 29, 2570-2578.
- Bokhari, Ali R Murrell, George A C. (2012). The role of nitric oxide in tendon healing. Journal of Shoulder and Elbow Surgery, 21, 238-244.
- Lin, J Wang, M Wei, A Zhu, W Murrell, G A C. (2001). The cell specific temporal expression of nitric oxide synthase isoforms during Achilles tendon healing. Inflamm. res., 50, 515-522.
- Vance, Carol G.T. Dailey, Dana L. Rakel, Barbara A. Sluka, Kathleen A.. (2014). Using TENS for pain control: the state of the evidence. Pain management, 4, 197-209.
- Dong-mei Jin, Yun Xu, Deng-feng Geng, Tie-bin-Yan. (2010). Effect of transcutaneous electrical nerve stimulation on symptomatic diabetic peripheral neuropathy: A meta-analysis of randomized controlled trials. PlumX Metrics, 89, 10-15.
- Sahdeo Prasad,Amit K. Tyagi, Bharat B. Aggarwal. (2014). Recent Developments in Delivery, Bioavailability, Absorption and Metabolism of Curcumin: the Golden Pigment from Golden Spice. Cancer research and treatment, 46, 2-18.
- Martínez-Augustin O, Sánchez de Medina F Departamento. (2004). Arginina, óxido nítrico y función endotelial. Ars Pharm, 45, 303-317.
- Nørregaard, Authors Jesper Gram, Martin Vigelsoe, Andreas Wiuff, Caroline Birk, Anja. (2014). Effects of different vitamin-C enriched collagen derivatives on collagen synthesis Dana. february 14, 2018, de International Journal of Sport Nutrition and Exercise Metabolism Sitio web: https://doi.org/10.1123/ijsnem.2018-0385.





