
The butt wink produced by the gluteus is a pelvic retroversion that we perform in most cases due to a shortening of the main hip flexors such as the rectus anterior quadriceps and the iliac psoas. This musculature is not fully relaxed and prevents the hip from remaining in a neutral position by exceeding a certain joint range in hip flexion. The lack of ankle dorsiflexion also influences the appearance of the butt wink. In most cases, when we perform a deep squat below 90º, the retroversion usually occurs and this retroversion leads the lumbar spine to a flexion. This flexion of the lumbar spine could increase the risk of injury. For this, we propose a reciprocal inhibition technique produced by whole-body electrostimulation to keep the hip and lumbar spine in a neutral position and avoid that butt wink when exceeding a certain joint range and see its effects later, if they are maintained without electro or no.
We propose a practical case where we will first analyze the mobility of the ankle dorsiflexion and see if it is optimal or not. Secondly, we will focus on the hip muscles to see if you have a shortening of the hip flexors (iliac psoas and rectus quadriceps) and correct the butt wink. Third and last, as a complementary technique to the correction of the “butt wink”, we will focus on correcting the knee wink or knee valgus produced by internal hip rotation.
Musculature responsible for the butt wink
The musculature responsible for the butt wink can be the plantar flexors of the ankle such as the soleus and calves, which can limit the ankle dorsiflexion. On the other hand, we have the iliac psoas and rectus anterior hip muscles and their shortening can produce a retroversion of the hip (butt wink) in the squat.
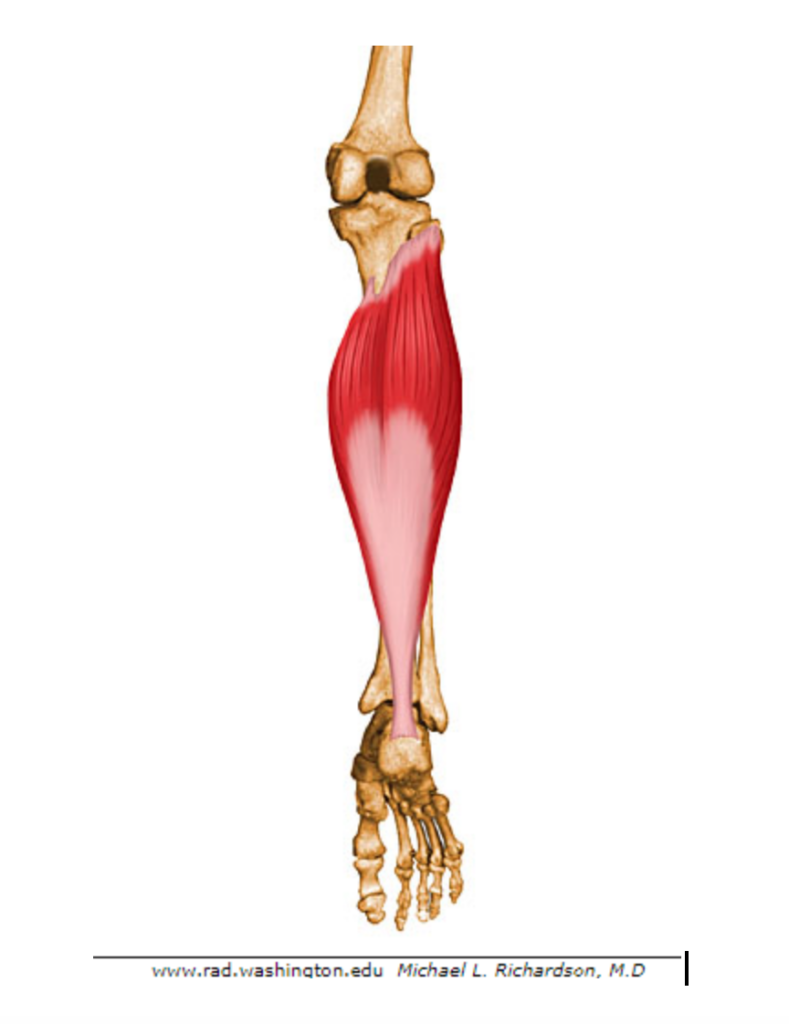
Soleus
The soleus or triceps sural is shaped like a sole. Their lateral faces protrude to the sides of the lower part of the cufflinks. This muscle originates below the posterior oblique line of the tibia, head of the fibula, and a posterior proximal third of the fibula. Its insertion occurs on the tibia at its medial border. Its function is the extension of the ankle or plantar flexion.
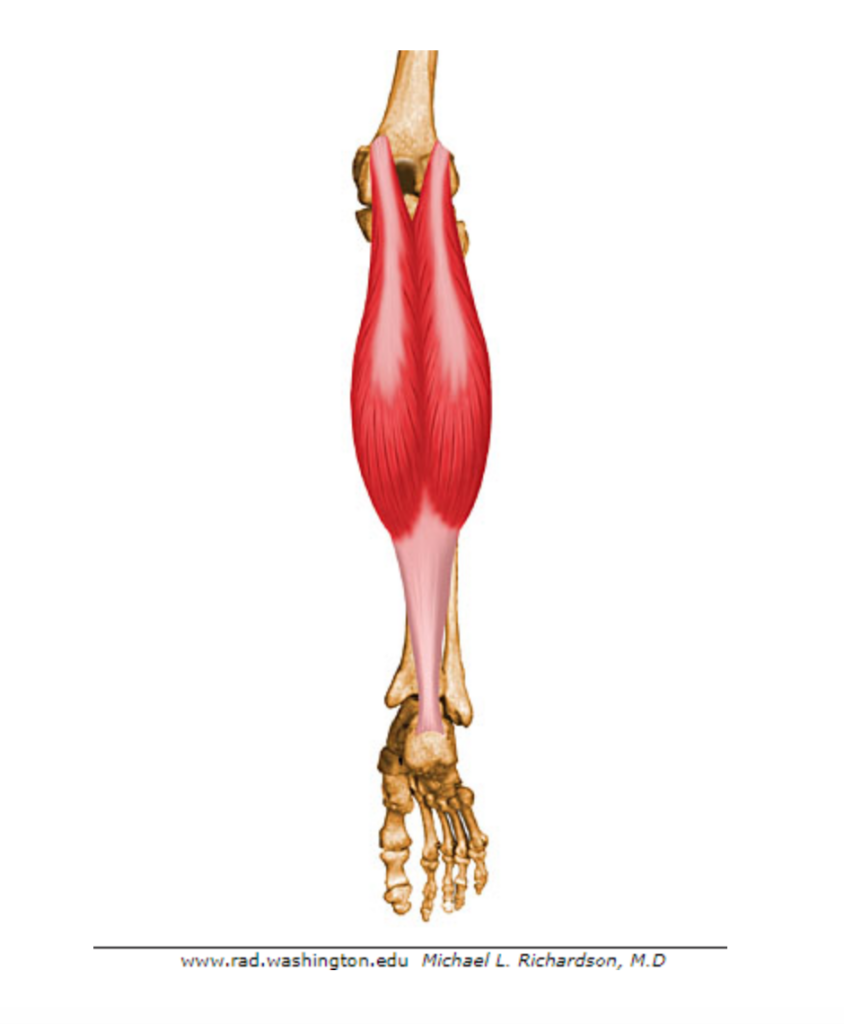
Cufflink
The twin is made up of an external head and an internal one, of which the internal one is the highest and thickest. They are also called Gastrocnemius. The internal head of this muscle originates from the posterior superior aspect of the medial femoral condyle, much higher than the origin of the external twin. On the other hand, the external head originates from the posterior superior aspect of the external femoral condyle. The two heads make a curvilinear trajectory to form the lower popliteal rhombus and insert into the posterior aspect of the calcaneus. Its function on the knee is to stabilize the femur, to prevent it from unbalancing forward in flexion movements, it also has the function of flexor whenever the knee is extended and the ankle flexed. On the ankle it has the function of extensor with tendency to the inversion.
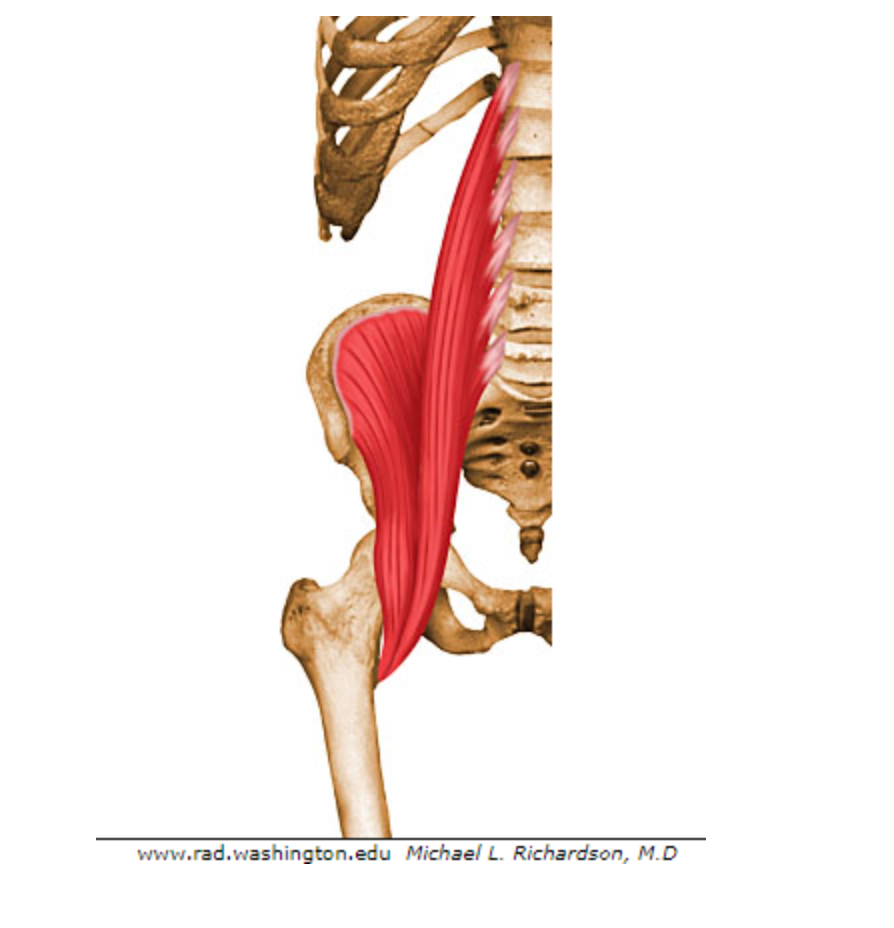
Iliac Psoas
The Psoas is a biarticular muscle that is composed of two muscles: the iliac and the psoas, which in turn could be divided into psoas major and psoas minor.
The psoas major attaches proximally to the body of the T12, in all lumbar vertebrae and through thinner fascicles, in the transverse processes of the lumbar vertebrae. More distally, it passes anterior to the sacroiliac joint and continues along the pelvic rim, passing anteriorly through the roof of the hip joint.
On the other hand, the psoas minor that originates from the anterolateral aspect of T12 and the first two lumbar areas and inserts on the pectineal line.
Finally, the iliac muscle originates from the upper two thirds of the inner surface of the iliac fossa, all the way to the lesser trochanter.
The action of the psoas is flexion of the hip and flexion of the lumbar spine.
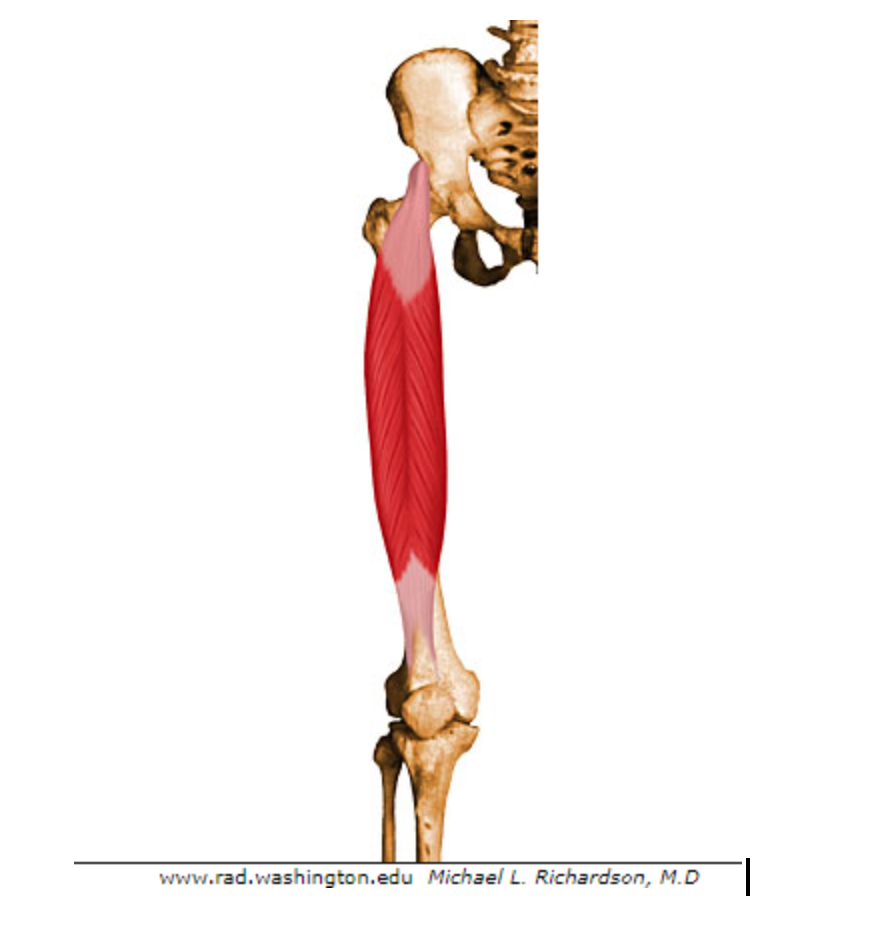
 Rectus anterior quadriceps
Rectus anterior quadriceps
The rectus anterior is a portion of the biarticular quadriceps muscle, originating from the anterior inferior iliac spine and attaching to the superior border of the patella. From there, it continues along the anterior face of the patella until reaching the anterior tibial spine through the patellar tendon. The action of this muscle on the hip is flexion with a slight tendency to abduction and pure extension on the knee.
Reciprocal inhibition
The ‘’ Sherrington Principle ’’ or reciprocal inhibition occurs when a muscle contracts due to a nervous action, said muscle would be the agonist and, on the contrary, the antagonist muscle receives a simultaneous signal that inhibits it. For example, if we perform a gluteal contraction, its antagonist, the iliac psoas, relaxes.
Sherrington’s laws are those that govern mechanical activity during muscle contraction and are:
- First Law: A muscle in its maximum stretch will suffer as a reflex effect a maximum contraction, this means that a muscle in an extreme stretch the muscle contracts with greater power than in normal working conditions.
- Second Law: When an agonist muscle contracts by successive reverse innervation, the antagonist muscle will relax to the maximum. However, the antagonist muscle will be prepared to perform a more effective contraction. This second law is what we will apply in the intervention of this “butt wink” correction method using full body electrostimulation (WB-EMS).
Reciprocal inhibition with EMS
Electrostimulation (EMS) of the lower extremities causes muscle contractions by activating fibers, which can modulate the excitability of the central nervous system.
In a study it was seen that the application of EMS for 60 seconds with a medium frequency protocol (40 Hz), with a pulse width of 300 µs and a motor threshold intensity can produce an inhibition in spinal reflexes for 15 minutes [ 3]. Knowing this, we can think that EMS can be very useful to provoke a reciprocal inhibition and to correct the ” butt wink ”.
Intervention of the practical case
Intervention on the ankle
We will perform a dorsiflexion on a wall measuring the distance of the joint range (from the wall and tiptoe). Once we have the measurement, we will connect the electrostimulation in the soleus and calf with a frequency of 40 Hz, 300 µs of pulse width with a motor threshold intensity for 60 seconds. After the electrostimulation work cycle, we will do the dorsiflexion again and see if the joint range has increased, how much this joint range has increased, and for how long this improvement is maintained.
Intervention on the hip
We will perform a squat without full body electrostimulation (WB-EMS) analyzing the joint range point where the butt wink is given. Once the point has been analyzed, we will connect the electrostimulation and perform two phases:
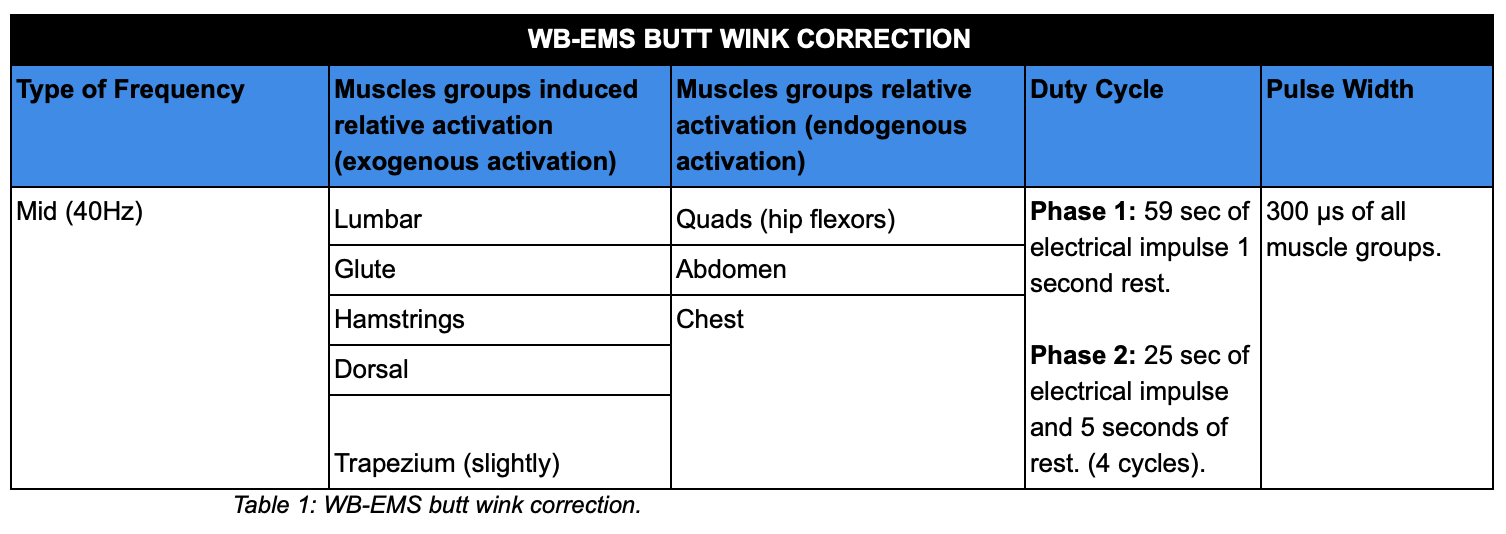
- Phase 1: We will connect electrostimulation only in the muscles that we want to inhibit. The electrostimulation protocol will be at a frequency of 40 Hz, with a pulse width of 300 µs, with a motor threshold intensity for 60 s. This should produce an inhibition of the spinal reflexes connected to said musculature for at least about 15 minutes. This phase will be performed in the supine position.
- Phase 2: In this phase we will connect the full body electrostimulation (WB-EMS) while the subject will perform the squat within the electrical impulse. The WB-EMS protocol similar to the previous phase, the only difference will be the dutty cycle of the electrical impulse, which will be 25 seconds of work and 5 seconds of rest and the intensity threshold that in the muscles that we want to inhibit will be at a threshold sensitive and the muscles that we want to coerce will be at a motor threshold. There will be 4 sets of squats. In this way we will exogenously activate those muscles that have less endogenous activation (inhibited muscles), increasing the intensity of the electrical impulse of said muscles, on the other hand, we will reduce the intensity of the antagonist muscles. In this way, it will be possible to relax the muscles that have greater endogenous activation that is responsible for the action of the ” butt wink ” by performing a reciprocal inhibition. When this reciprocal inhibition occurs, we will be able to keep the hip and spine in a neutral position by squatting with greater joint range. At the end of the intervention, check if the inhibition is maintained without electrostimulation (Table 1).
Intervention on the knee
For this intervention, our subject will perform a squat without connecting electrostimulation. In the squat we will analyze the knee wink (internal hip rotation). Once this knee wink has been analyzed, we will connect the electrostimulation in the stabilizing knee muscle groups such as the gluteus, quadriceps and hamstrings and we will analyze if that knee wink stops. Also, we will give feedback to the subject so that he can correct the knee wink endogenously, this feedback will be given both in the phase without electrostimulation and in the phase with electrostimulation. The electrostimulation parameters will be 40 Hz, with a pulse width of 300 µs, with an intensity of a motor threshold and a duty cycle of 25 seconds of electrical impulse and 5 seconds of rest. Finally, after four cycles of electrostimulation we will repeat the squat without electrostimulation and we will see if the hip wink has been corrected.
Bibliography:
- Sajko, Sandy Stuber, Kent. (2009). Psoas Major: a case report and review of its anatomy, biomechanics, and clinical implications.. The Journal of the Canadian Chiropractic Association, 53, 311-8.
- Robert E. McAtee, Jeff Charland. (2000). ESTIRAMIENTOS FACILITADOS. Los estiramientos de FNP con y sin asistencia. España: Editorial Paidotribo.
- Matija Milosevic, Yohei Masugi, Hiroki Obata, Atsushi Sasaki, Milos R. Popovic, Kimitaka Nakazawa. (2019). Short-term inhibition of spinal reflexes in multiple lower limb muscles after neuromuscular electrical stimulation of ankle plantar flexors. Experimental Brain Research, 237, 467-476.





